Cases scheduled for neck surgery were classified as having modic type I changes and biopsied for Propionibacterium Acnes Infection during surgery.
no modic changes – 20% were positive for p.acne infection
modic changes – 54% positive were positive for p.acne infection
AJNR Am J Neuroradiol. 2018 Sep;39(9):1764-1767. doi: 10.3174/ajnr.A5741.
Association between Type 1 Modic Changes and Propionibacterium Acnes Infection in
the Cervical Spine: An Observational Study.
Georgy MM et al
https://www.ncbi.nlm.nih.gov/pubmed/30139754
This is nothing new
Repeated studies demonstrated you could grow Propionibacterium Acnes out of back or neck disc with modic changes ( one study did not find it mattered what type).
I wrote about it here:
Chronic Neck and Back Pain Might Be a Treatable Infection
http://painmuse.org/?p=2342
Since that writing other studies have found a bacterial presence:
Zhou, Zezhu, et al. Relationship between annular tear and presence of Propionibacterium acnes in lumbar intervertebral disc. European Spine Journal 24.11 (2015): 2496-2502.
https://link.springer.com/article/10.1007/s00586-015-4180-y
1/3 a samples with annular tear were positive for Propionibacterium acnes while there was only 1 case positive in controls
Another study:
Capoor, Manu N., et al. “Prevalence of Propionibacterium acnes in intervertebral discs of patients undergoing lumbar microdiscectomy: a prospective cross-sectional study.” PLoS One 11.8 (2016): e0161676.
prevalence of discs with abundant P. acnes was 11% (did not take modic changes into consideration
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0161676
Yet another study:
Aghazadeh, Javad, et al. “Modic changes in the adjacent vertebrae due to disc material infection with Propionibacterium acnes in patients with lumbar disc herniation.” European Spine Journal 26.12 (2017): 3129-3134.
https://link.springer.com/article/10.1007/s00586-016-4887-4
16S rDNA gene [for Propionibacterium acnes] was identified in 46 (38.3%) disc samples. Moreover, 36/46 patients with P. acnes in their sample had Modic changes.
Yet another:
Capoor, Manu N., et al. “Propionibacterium acnes biofilm is present in intervertebral discs of patients undergoing microdiscectomy.” PloS one 12.4 (2017): e0174518.
“Bacteria were cultured from 162 discs (44%), including 119 cases (32.3%) with P. acnes. In 89 cases, P. acnes was cultured exclusively; in 30 cases, it was isolated in combination with other bacteria (primarily coagulase-negative Staphylococcus spp.) Among positive specimens, the median P. acnes bacterial burden was 350 CFU/g (12 – ~20,000 CFU/g). Thirty-eight P. acnes isolates were subjected to molecular sub-typing, identifying 4 of 6 defined phylogroups: IA1, IB, IC, and II. Eight culture-positive specimens were evaluated by fluorescence microscopy and revealed P. acnes in situ. Notably, these bacteria demonstrated a biofilm distribution within the disc matrix. P. acnes bacteria were more prevalent in males than females (39% vs. 23%, p = 0.0013).
Conclusions
This study confirms that P. acnes is prevalent in herniated disc tissue. Moreover, it provides the first visual evidence of P. acnes biofilms within such specimens, consistent with infection rather than microbiologic contamination.”
Yet another:
Yuan, Ye, et al. “Histological identification of Propionibacterium acnes in nonpyogenic degenerated intervertebral discs.” BioMed research international 2017 (2017).
http://downloads.hindawi.com/journals/bmri/2017/6192935.pdf
16/76 cases positive for P. acne and 7 were visible on histological staining
Yet another:
Shifflett, Grant D., et al. “Microbiologic profile of infections in presumed aseptic revision spine surgery.” European Spine Journal 25.12 (2016): 3902-3907.
https://link.springer.com/article/10.1007/s00586-016-4539-8
Of 565 revision surgery cases, 19.4% positive for either P. acne or staphlococcus. Most common diagnosis was pseudoarthrosis. So 1/5 are positive.
Yet another:
Javanshir, Naghmeh, et al. “The distribution of infection with Propionibacterium acnes is equal in patients with cervical and lumbar disc herniation.” European Spine Journal 26.12 (2017): 3135-3140.
https://link.springer.com/article/10.1007/s00586-017-5219-z
“P. acnes infection was detected in nine patients (36%) with cervical disc herniation and 46 patients (38.3%) with lumbar disc herniation”
Yet another:
Yuan, Ye, et al. “Association between chronic inflammation and latent infection of Propionibacterium acnes in non-pyogenic degenerated intervertebral discs: a pilot study.” European Spine Journal (2017): 1-12.
https://link.springer.com/article/10.1007%2Fs00586-017-5363-5
15/76 disc – “Latent P. acnes infection was associated with chronic inflammation in degenerated intervertebral discs, especially in the samples with visible bacteria in histology, which manifested as increased numbers of cytokines and neutrophils. Discs with P. acnes infection had much severer disc degeneration and P. acnes-associated chronic inflammation may be the reason.”
and Another:
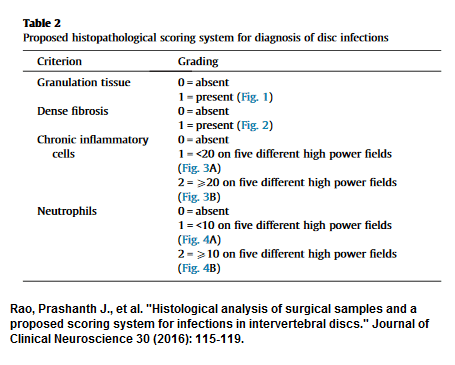
Rao, Prashanth J., et al. “Histological analysis of surgical samples and a proposed scoring system for infections in intervertebral discs.” Journal of Clinical Neuroscience 30 (2016): 115-119.
https://www.researchgate.net/profile/Ralph_Mobbs/publication/277909497_Histological_Analysis_of_Degenerate_Discs_Disc_Study-is_there_Support_for_Infection_as_a_Possible_Etiology_for_Disc_Degeneration/links/5738256d08ae298602e1af9b/Histological-Analysis-of-Degenerate-Discs-Disc-Study-is-there-Support-for-Infection-as-a-Possible-Etiology-for-Disc-Degeneration.pdf
They proposed scoring but had to resort to histological findings:
Chen, Yilei, et al. “Low virulence bacterial infections in cervical intervertebral discs: a prospective case series.” European Spine Journal (2018): 1-10.
https://link.springer.com/article/10.1007/s00586-018-5582-4
25% positive rates
Yet there was a negative case looking for bacterial riobosomal rna:
Alamin, Todd F., et al. “Ribosomal PCR assay of excised intervertebral discs from patients undergoing single-level primary lumbar microdiscectomy.” European Spine Journal 26.8 (2017): 2038-2044.
https://link.springer.com/article/10.1007/s00586-017-5141-4
Comment –
- reminds me of post-partum infection and H. pylori infection denial stage in medical practice. It would appear maybe 1/5 cases have infection – either P. acne or Staph.
- Chronic clavulin 500 mg tid (might need some loperamide to control the diarrheal effects of clavulanic acid) administration was found to drop chronic back pain by 2/10 over 3 months use.
Albert, Hanne B., et al. “Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): a double-blind randomized clinical controlled trial of efficacy.” European Spine Journal 22.4 (2013): 697-707.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3631045/pdf/586_2013_Article_2675.pdf - I have toyed with idea of using azithromycin – one dose for can was 150 mg x2 three times weekly:
Kapadia, Naseema, and Abu Talib. “Acne treated successfully with azithromycin.” International journal of dermatology 43.10 (2004): 766-767.
https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-4632.2004.02058.x
- I would use in in post surgical cases and modic (not specifically I or II) changes. “Proscribing Wisely” initiative tells us to avoid unnecessary imaging but obviously hasn’t heard of this condition..
addendum:
Trials. 2017 Dec 15;18(1):596. doi: 10.1186/s13063-017-2306-8.
Antibiotic treatment In patients with chronic low back pain and Modic changes
(the AIM study): study protocol for a randomised controlled trial.
Storheim K et al
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5732434/
- running a trial to test antibiotic use for back pain
- Since P. acne is not a beta lactam bacteria, they are using amoxicillin 750 mg tid which makes more sense and would cause considerable less side effects.
