Continuous pain of tooth without obvious cause is called Atypical Odontalgia. Up until now it has been poorly treated. Now injection of botulinum can achieve at least 50% reduction in pain. It requires injecting gums between affected teeth and areas of referral – including lips and palate if necessary.
J Pain Res. 2018 Aug 23;11:1583-1588. doi: 10.2147/JPR.S169701. eCollection 2018.
OnabotulinumtoxinA injections for atypical odontalgia: an open-label study on
nine patients.
García-Sáez R et al
https://www.dovepress.com/onabotulinumtoxina-injections-for-atypical-odontalgia-an-open-label-st-peer-reviewed-fulltext-article-JPR#
- Their theory involves peripheral sensitization of periodontal nerve plexus
- piloted 4 cases and went on to do 5 more = 9 cases
- mean maximal pain was 8/10
- all had “phantom pains” from missing teeth
- Used Onabotulinumtoxin A (OnabotA)
- 100 units in 2 mls = 5 units/0.1ml
- Using 30 gauge needle injected 0.05 ml = 2.5 u each site
- Injected “dental alveoli of missing teeth” – ie the hole
- Injected in interdental papilla gingiva :


Then inject several sites on gingival mucosa (maybe between other teeth sore etc
Then inject adjacent pain referring gum and palate areas
[most pics directly from article]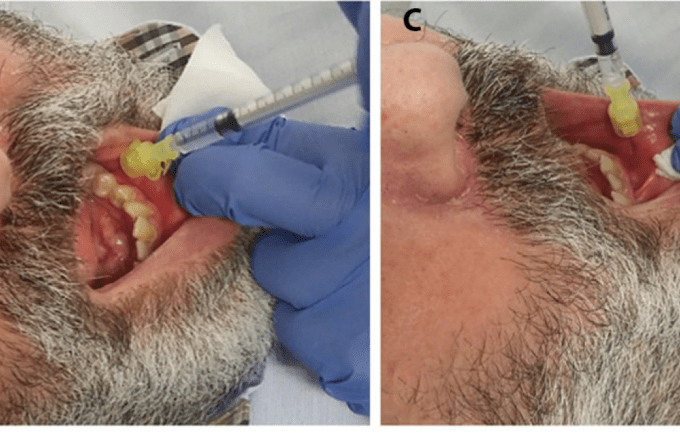
Injected up to 12 sites = max dose 30 u – mean was 8 sites per patient – minimum 4 sites
repeat procedure q3 months
- Over 50% relief with max pains 0-3/10
- one all better, 4 intermittent pain, and rest mild continuous pain
- duration effect 2-6 months
Comment – I have a case of occipital neuralgia I first inject with botulinum and the follow up 1-2 weeks later with semi-neurolytic 5% lidocaine injections. The bolulinum renders nerves more sensitive to the semineurolytic effects. I Think they could have capitalized on the botulinum by following up with 5% lidocaine injections. Nonetheless, they have preformed a miracle for cases sometimes just tossed away as “nuts”.
Addendum:
New article discussing orofacial pains, some after dental implants, after facial nerve reconstruction, or just atypical orofacial pains – the former 2 did well with botulinum but not the latter.
Maxillofac Plast Reconstr Surg. 2018 Aug 6;40(1):21. doi:
10.1186/s40902-018-0159-z. eCollection 2018 Dec.
Treatment of non-odontogenic orofacial pain using botulinum toxin-A: a retrospective case series study.
Kim SY et al
https://www.ncbi.nlm.nih.gov/pubmed/30206537
- describe atypical facial pain as diffuse pain deep in tissues without obvious cause ranging from dull, tingling, sharp or throbbing. Treatment is often unsatisfactory.
- case 1 – upper lip and palate burning and throbbing – used 250 u Dysport into right upper anterior gingiva and repeated 3 month later with no pain thereafter
- case 2 – intermittent severe pain after facial reconstruction – at 3 month intervals: 25 u Innotox into left face and left masseter; repeat left low lid and zygoma; 3rd into stylomastoid foramen – markedly reduced pain
- Cases after dental implant surgery responded well BTX-A varied from 20 – 200 u a dose
- 2 cases of atypical facial pains did NOT do well
- transient facial asymmetry or unbalance occurred but was not a major problem.
- Their conclusion was subjects that had pain from traumatic trigeminal neuralgias from dental implants or facial nerve damage – did well – more into gingiva vestibule and lip, masseter and temporalis
- But atypical facial pains did not respond
