Reading through a German review of CRPS some simple measures became obvious -Prednisone, Alendronate, high dose Gabapentin, DMSO, and Ketamine
Unfallchirurg. 2018 Sep 14. doi: 10.1007/s00113-018-0544-1 in press
[Complex regional pain syndrome].
Herlyn P.
https://www.ncbi.nlm.nih.gov/pubmed/30218165
Physiotherapy
This is usually quite involved and involves desensitizing structures by graded exposure. However, early on, mirror image therapy was found helpful:

In:
McCabe, C. S., et al.
A controlled pilot study of the utility of mirror visual feedback in the treatment of complex regional pain syndrome (type 1).
Rheumatology 42.1 (2003): 97-101.
https://academic.oup.com/rheumatology/article/42/1/97/1779776
“Subjects were asked to attend to the non‐reflective surface for a period of 5 min and exercise their non‐painful limb and, if possible, their painful limb in a congruent manner. All subjects were asked to attempt to perform similar exercises: flexion–extension cycles of the relevant body parts. The range of movement and speed of these exercises was dictated by the subject’s pain.”
no more than 10 minutes at a time and as frequent as they liked.
Results: “All three subjects with early CRPS (≤8 weeks) reported a striking reduction in their pain VAS during and after visual feedback of their moving, unaffected limb as provided by the mirror. A marked analgesic effect was observed within a few minutes of mirror use, followed by an abrupt return of pain when the mirror was removed initially. With repeated use (four to nine times daily, week 1), the period of analgesia extended progressively from a few minutes to hours, requiring less mirror use over the 6‐week study period. At 6 weeks there was a reversal of vasomotor changes as measured by IRT, a return to normal function and no pain at rest or on movement. All three subjects felt they no longer required analgesic relief from the mirror and had stopped prior to assessment at 6 weeks (case 3, week 4; cases 1 and 2, week 6).”
Prednisone
Early can be life changing. A Canadian article queries why is this not done early:
•Pain Research and Management 2016 (2016). Winston, Paul. Early treatment of acute complex regional pain syndrome after fracture or injury with prednisone: why is there a failure to treat? A case series. Pain Research and Management 2016 (2016).
http://downloads.hindawi.com/journals/prm/2016/7019196.pdf
Article suggests a few weeks might be enough though a study of post stroke CRPS found TWO months was necessary:
Kalita, Jayantee, et al. Long-term prednisolone in post-stroke complex regional pain syndrome. Pain physician 19.8 (2016): 565-574
http://www.painphysicianjournal.com/current/pdf?article=MzEwNA%3D%3D&journal=100
I use 50 mg/day for 2-3 weeks then gradually taper over 2 month. You do have to warn them they are at risk of hip osteonecrosis.
Biphosphonates
Early in course, IV Pamidronate can give good results.
http://painmuse.org/?p=54
However, later results are not good:
Pain Med. 2017 Jun 1;18(6):1131-1138. doi: 10.1093/pm/pnw207.
Predictors of Responsiveness to Bisphosphonate Treatment in Patients with Complex Regional Pain Syndrome Type I: A Retrospective Chart Analysis.
Varenna M et al
https://academic.oup.com/painmedicine/article/18/6/1131/2924769
“Conclusion. Early disease, fracture as a predisposing event, and “warm” disease subtype are predictors of responsiveness to bisphosphonate treatment in patients with CRPS-I.”
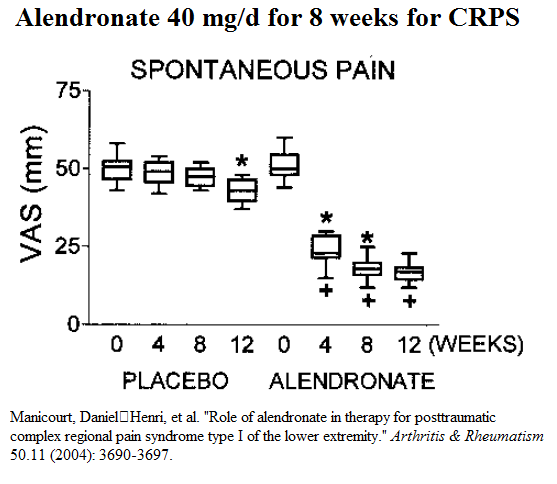
So, later in its course, probably better to just use High dose oral alendronate:
Manicourt, D. H., Brasseur, J. P., Boutsen, Y., Depreseux, G., & Devogelaer, J. P. (2004).
Role of alendronate in therapy for posttraumatic complex regional pain syndrome type I of the lower extremity.
Arthritis & Rheumatism, 50(11), 3690-3697.
https://onlinelibrary.wiley.com/doi/epdf/10.1002/art.20591
- CRPS type 1 – 20 in active and 20 in placebo
- 40 mg of alendronate – “taken with a full glass of water upon arising for the day (after an overnight fast),
and patients were instructed to remain in an upright position for 30 minutes prior to consuming the first food or beverage of
the day.” - given for 8 weeks
- Results:
Gabapentin ?
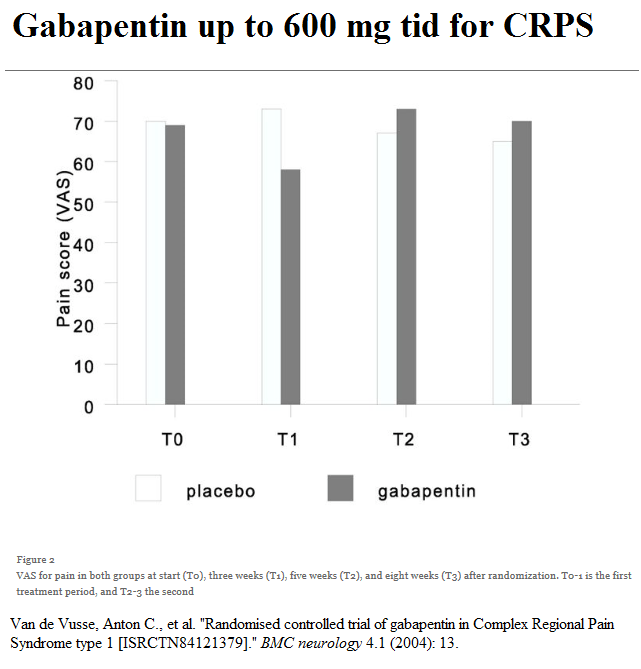
I’m not a big fan of gabapentin; In the one study of use in CRPS it dropped pain temporarily by 1 point only. Argument could be made that 1800 mg/day is not the full 2400 mg that could be used. People brag that it is used in neuropathic pain without realizing a trial of efficacy on combination therapy for neuropathic pain only achieve clinically relevant benefit in 23.7% of cases.
Moulin, Dwight E., et al.
Long-term outcome of the management of chronic neuropathic pain: a prospective observational study.
The Journal of Pain 16.9 (2015): 852-861.
http://www.jpain.org/article/S1526-5900%2815%2900703-8/fulltext
One study using 1800 mg was mediocre:
Pushing the dose to 2400 mg does seem to have benefits as a study on traumatic nerve injuries demonstrated:
Gordh, Torsten E., et al.
Gabapentin in traumatic nerve injury pain: a randomized, double-blind, placebo-controlled, cross-over, multi-center study.
Pain 138.2 (2008): 255-266.
https://www.sciencedirect.com/science/article/pii/S0304395907007518
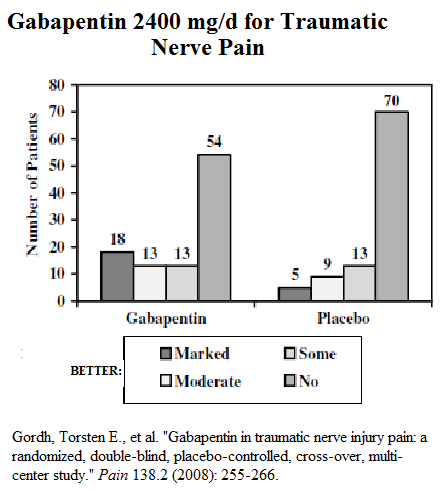
Seems that one has to push the dose of this and that will not always be possible.
However another study on neuropathic pain at 2400 mg got the following:
Pain. 2002 Oct;99(3):557-66.
Gabapentin in neuropathic pain syndromes: a randomised, double-blind, placebo-controlled trial.
Serpell MG; Neuropathic pain study group
http://www.ncbi.nlm.nih.gov/pubmed/12406532
- large enough 153 in gabapenin; 152 in controls

Not at all promising but here are subgroups that are responders.
Dimethylsulfoxide (DMSO) topically –
actually easier than one would think because available as a horse liniment at a horse supply store (one I’ve seen looks like a deodorant roll-on). Can cause irritation sometimes so may have to use a steroid to area as well.
Ketamine
The best results have been with higher dosage iv programs that run for days but these are inpatient and not readily available. There was a study from Texas where they were able to simulate IV ketamine by giving small doses every 10-15 mg into deltoid muscle. They found if given daily to start, they could get a great reduction in neuropathic pain level.
http://painmuse.org/wp-content/uploads/anodynehealth.pdf
I’ve done a project where is was given longterm and found it can give people some of their life back. It improves mood and well as pain. Unfortunately, in CRPS it only lasts 0.5 – 1.5 days. However, subjects can plan their life around the shots and get a bit of life out of it. It is also reassuring that if things get too bad, they can always go for a shot. People typically have shots 1-2 times a week. I presented this poster to the CPS 2017;
https://painmuse.org/wp-content/uploads/Poster-CPS-2017-ketaminefinal-2.pdf
ketamine can also be used topically with varying results in PLO gel at concentrations of 1-15%.
Kopsky, D. J., et al.
Analgesic effects of topical ketamine.
Minerva Anestesiol 81.4 (2015): 440-449.
https://s3.amazonaws.com/academia.edu.documents/37397596/Kopsky__Keppel_Hesselink__et_al_ketamine_analgesia_rev._15.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1539142877&Signature=mVc9d%2FD%2B3yIEM5oP8knYGQnFNt4%3D&response-content-disposition=inline%3B%20filename%3DAnalgesic_effects_of_topical_ketamine.pdf
Various blocks
From there, one goes to various blocks – but this might not be available everywhere.
Spinal Stimulators:
are often used as a last resort. However the late Dr. K. Kumar, one of the founders of this procedure (and from my town…), was of the opinion it worked best when given early – why has that not caught on?
