I have seen a case that I read in:
http://butmaybetomorrowkd.blogspot.com/
I have 4 patients that she is a composite of so I’d like to go over what made a difference to them. Most of the treatments are out of the box treatments that can be helpful.
1) chronic severe pains nonspecific Rx There is a composite of factors that can help that can make a difference but work best in groups of three.
Included are:
- vitamin D3 minumum 4000 u/day. I take 50,000 weekly for its anticancer properties and high levels are also associated with covid protection
read: Vitamin D – Could High Doses Help Pains? http://painmuse.org/?p=4168
- Vitamin B12 high subcut dose read:
Vitamin B12 Injections For Chronic Pain
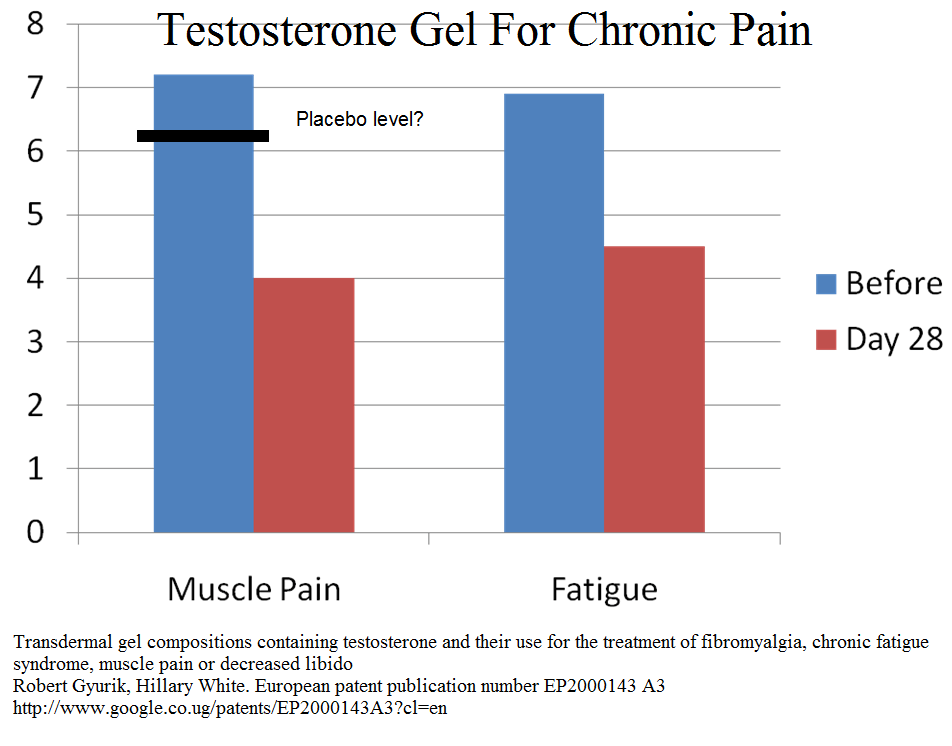
http://painmuse.org/?p=7098 - Testosterone (gel 0/2-0.3 ml/day topical) (below study used 0.7ml/day though)
- Ketamine is a big one for all my severe cases and one of the few things that helps in CRPS. I helped pioneer a program initially in a doctors office and as the drowsiness becomes less at home with a reliable partner
read here: Office Ketamine For Chronic Pain Poster –
http://painmuse.org/?p=5611 - opioids -most can make headaches worse but you may get away with buprenorphine (butrans patches) or methadone because of kappa opioid atagonism
2) Chronic Regional Pain Syndrome Rx: – this disorder can respond to either: ( and subtle inflammatory conditions)
– high dose steroids – mentioned in
https://wordpress.com/post/newpainmuse.org/125
– Pamidronate – a bone building IV agent that works in CRPS and in some chronic inflammation issues:
I wrote about it here:
Pamidronate and Clodronate – hope for Reflex Sympathetic Dystrophy (aka CRPS) and Back Pain
http://painmuse.org/?p=54
and here:
Chronic Back Pain May Be a Pamidronate Infusion Treatable Disease – And Why Did It take 10 Years to Replicate That?
http://painmuse.org/?p=3002
It also works in subtle ankylosing spondylitis neck and back inflammatory conditions. I have one lady dismissed by rheumatologists but did well on ketamine and prednisone cortisone but I had to stop latter because of bone loss. IV infusions of pamidronate regained her pain control ( mentioned how to use for spondylitis in first link above)
3) Subcutaneous nerve pains – you do not get a “red Neck” without irritation to the skin nerves. There is a new treatment that invovles injecting the scar and the skin cervical dorsal nerve roots repeatedly with plain 5% dextrose sugar water repeatedly. It is called perineural injections.
I talked about it here:
Skin Nerve treatment in CRPS
http://painmuse.org/?p=7126
and here:
http://painmuse.org/?p=7131
best results are when it is combined with botulinum in skin:
Both Subcutaneous and Perineural Botulinum Treatments Advocated
http://painmuse.org/?p=3198
on the earlier neck image you can see red v-ing out from C6 right – likely C6 dorsal nerve root that comes up by spinal process medially and then v’s out.
subsequent to botulinum skin areas can be injected with 5% lidocaine with or without 20-50 ethanol alcohol to deaden skin nerves
4) Getting right out of box . There is a whole school of thought that particularly operated spinal areas in constant pain are populated with a low level infection of P. acne – the germ involved in acne.
I wrote about it here:
Chronic Neck and Back Pain Might Be a Treatable Infection
http://painmuse.org/?p=2342
and here:
Neck or Back Pain with MRI Modic Changes Could be Infection
https://wordpress.com/post/newpainmuse.org/55
I have one patient with neck ops and facet rhizotomies living with pain of 9.5/10 surviving with ketamine. I started him on Azithromycin 250 mg bid x 2 weeks then 250 mg 2-3 times a week. By 2 months his pain had dropped to 4-5/10 in am (he tends to overdo things as a result so higher later in day)
5) HIGH dose nabilone (4 mg) might help but needs high dose:
Elderly with Resistant Post Herpetic Neuralgia – What do You Do?
http://painmuse.org/?p=6800
6) Nerve blocks both stellate ganglion nerve blocks ( can be done repeatedly safely with just sugar water) – mentioned here:
https://downloads.hindawi.com/journals/bmri/2017/7920438.pdf
or superior sympathetic ganglion radiofrequency:
Koning, Henk M., et al. Percutaneous radiofrequency lesion of the superior cervical sympathetic ganglion in non-traumatic neck pain.
The Pain Clinic 12.4 (2000): 271-279.
https://s3.amazonaws.com/academia.edu.documents/42121361/Percutaneous_radiofrequency_lesion_of_th20160205-30232-1ljes4y.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1522649321&Signature=kRKaj6bbZq7uRx2%2Bc2fgnjGq%2BDA%3D&response-content-disposition=inline%3B%20filename%3DPercutaneous_radiofrequency_lesion_of_th.pdf
I discussed it here for headaches as well:
Refractory Migraine Eliminated by Pulse Radiofrequency to Superior Cervical Ganglion -Good for Chronic Neck Pain as well
7) Intramuscular Stimulation (IMS) I should have mentioned earlier because lifesaver for one subject like you. IMS is electrically needling cervical muslces with a special unit called a pointer plus that you can pulse. This is Dr. Gunn’s technique and he has a site here:
you can check for a practitioner near you as becoming common among physiotherapists.
I hope you find it useful
