Injecting 25% dextrose into various locations in TMJ joint (superior joint space, inferior joint space, retrodiscal tissue, and anterior capsule) X 4 they were able to determine place for best injections. For clicking reduction and reduced derangement – retrodiscal injection was best. For relief of pain – retrodiscal or inferior joint worked best.
Fouda, A. A.
Change of site of intra-articular injection of hypertonic dextrose resulted in different effects of treatment.
British Journal of Oral and Maxillofacial Surgery (2018) in press
https://www.sciencedirect.com/science/article/pii/S0266435618302560
- 72 cases randomized – 18 each
Positions:
- 1 – outer capsule – midpoint of condylar head with mouth wide open
- 2 – superior joint space – mouth closed – upper surface condyle marked first. Needle injected from bottom and aimed upward until upper TMJ surface touched.
- 3 – inferior joint – mark upper surface. Enter through upper surface aiming down until touch bottom of tmj joint touched
- 4 -retrodiscal- mouth wide open – space between condylar head and tragus of ear.
Procedure:
- 25% dextrose with mepivacaine 1.5 mls injected with 22 gauge needle
- Four injections – 0, 1, 2, 3 weeks
Results on pain:

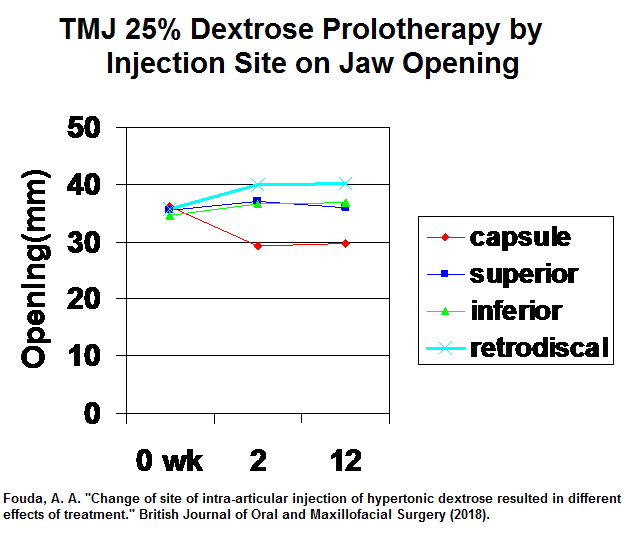
results on jaw opening:
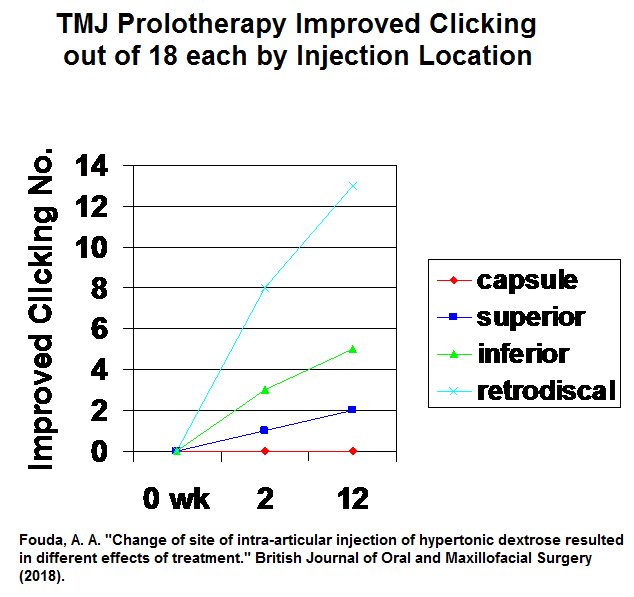
And by reduction in clicking:
- Finding that capsular injection reduced jaw opening might be useful in hypermobile joints.
- However for both pain reduction, increased jaw opening and decreased clicking, retrodiscal injection seemed best
Comment – I was taught TMJ inject by Ed Gherasim, an orthodontist in Regina now retired. He felt tearing of Posterior ligaments with anterior displacement of disc was common (lateral tearing with medial displacements too). He felt retrodiscal injection behind disc where ligament would have joined was the obvious target and this has borne true.
