Recently, I have been lucky enough to achieve control of a very bad headache sufferer using some advances I read. Using higher strength lidocaine; and frontally, pinpoint near nerve foramen injection for supra and infraorbital nerves. Recently an article found 9 mls of 1% lidocaine with 1 ml triamcinolone 40 mg (increased volume) helped 9/10 cluster headache, as well
Ideas:
Injecting suboccipital nerves had repeatedly been shown to make a difference – I wrote about it here:
50% Reduction in Migraines by Occipital Nerve Blocks
https://wordpress.com/post/newpainmuse.org/109
- Nerve blocks are easy as long as you are not planning to hit them head on (direct needle through to). Bend the needle maybe 30 degrees and run needle subcutaneously under skin parallel to direction of nerves. If you feel base of skull where it starts suboccipitally, the more tender and rope like spot will be it. Push down with your left index finger firmly and inject upward in direction nerve are tracking up. If you’ve held the tissue firm, the nerve will immediately react when you hit it and you can use this tinel’s to inject on the right spot.
- What I found is actually most tender is the 3rd subcutaneous occipital nerves – they come up just on the sides of the spinous process so you track up near midline. Injecting them is very important.

- using 5-10% lidocaine can give you a longer block:
J Pain Res. 2016 Sep 29;9:721-725.
Prolongation of greater occipital neural blockade with 10% lidocaine neurolysis:A case series of a new technique.
Kim DD et al
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5047742/
•60% reduction in migraine (10) or Occipital Neuraliga (3) for 148.05 +/- 98.87 days – However, you need to stick to 1 cc for 10% and 2 cc for 5% lidocaine. Scale down dose for smaller people.
Problem arises with the elderly:
Sahai-Srivastava, Soma, and Dawood Subhani.
Adverse effect profile of lidocaine injections for occipital nerve block in occipital neuralgia.
The journal of headache and pain 11.6 (2010): 519-523.
https://link.springer.com/article/10.1007/s10194-010-0244-x
he was very adamant that care has to be taken with elderly so I gave a 5% occipital shot using 1/2 dose – the reaction was very scary like an acute hypotensive episode – I don’t know if I will ever give occipital 5% shots to anyone over 60. - When I first started doing supraorbital and infraorbital blocks I asked if one should try to hit the foramen – I was told maybe not – but that is a mistake – hitting the nerve where it exits will give you a long lasting block
Perloff, Michael D., and Justin S. Chung.
Urgent care peripheral nerve blocks for refractory trigeminal neuralgia.
The American journal of emergency medicine 36.11 (2018): 2058-2060.
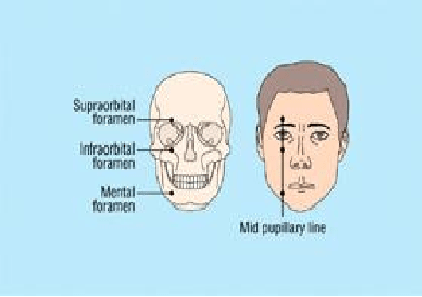
“30 g needle was inserted localizing to the supraorbital, infraorbital, and mental foramens. 0.5 mL of 0.25% bupivicaine:1% lidocaine was injected locally at all three foramens” –
– for Trigeminal Neuralgia Six of nine patients had lasting pain relief (1–8 months)
– I have used this for frontal pain in chronic severe headaches and after 1-2 goes they say the front is fine.
– the site is mid pupil vertical position just up or down – you can feel the depression where nerve comes out
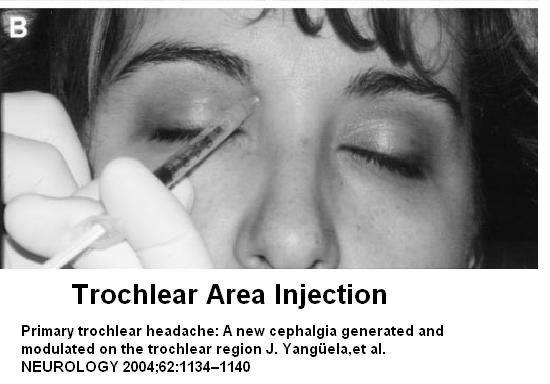
- If the trochlear fossa is tender (inner – upper orbit, then inject some cortisone in it will help as could be trochlear nerve headache:
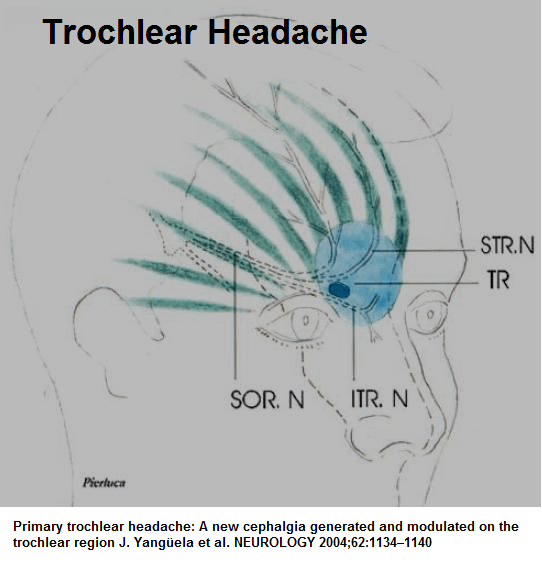
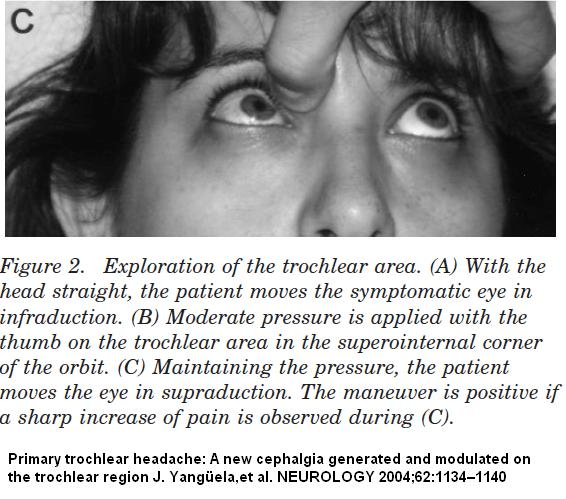
You can confirm it’s a problem by pressing over trocheal nerve area and have them look up – it should hurt more:
Using a shot 25 gauge needle, injecting 10-40 mg triamcinolone can eliminate it (relapses do occur though)
High volume occipital injection has recently veen shown to get a better block:
Headache. 2019 Jan;59(1):56-62. doi: 10.1111/head.13394.
High-Volume Anesthetic Suboccipital Nerve Blocks for Treatment Refractory Chronic Cluster Headache With Long-Term Efficacy Data: An Observational Case Series Study.
Rozen TD
https://www.ncbi.nlm.nih.gov/pubmed/30144049
Cluster headaches are injected with steroid as well. Results with low volume (typically 1-3 mls) are here:
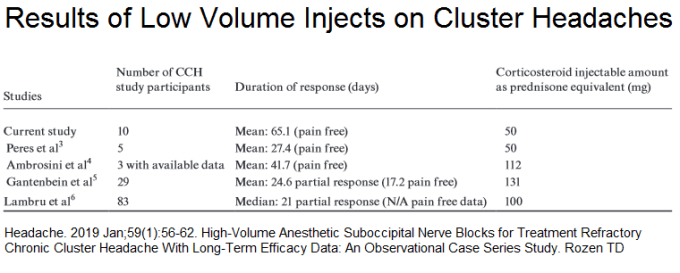
response rates were not usually great with low volume:
peres – 1/3
ambrosini – all 3 responded
Gantenbein – 29.9 painfree
Lambru – pain freedom of 15 days in 31%, 30 days in 15%, and 90 days in
2%. One patient remained pain free for 150 days
so it looks like response rate is 1/3 in low volume
High volume Cluster injection technique:
- single injection of 9 mL of 1% lidocaine and 1 mL of triamcinolone 40 mg injected on the side of CH pain
- location was in the suboccipital fossa at a point 1/3 laterally along an imaginary line from the inion to the mastoid process.
- Needle was inserted to the skull base and once the bone was touched, the injection was completed without deviation of the needle from side to side.
- Area of volume-based swelling was noted in the suboccipital region post procedure.
- Tenderness at the suboccipital injection location was not needed or required.
- Repeat injections -intervals of at least 4 weeks
- results – 9/10 responded – average duration 10.3 weeks
- cluster non-responders went on to:
-patient 3 – GON stimulator and was followed for 2 years after stimulator placement.
– Patient #9 – partial response to radiofrequency ablation of C2 dorsal root ganglia (DRG) and sphenopalatine ganglion (SPG) with lowered CH pain intensity but nochange in attack frequency
– Patient #10 has had significant improvement with combined radiofrequency ablation of the SPG and C2 DRG
si - side effects – sadly one with frequent injections developed avascular necrosis of hip
Comment -I hope people find insights helpful
