It looks like the only agents to maybe survive are topical amitriptyline and gabapentin and hormones estrogen and testosterone.
Here are a list of many of the studies:
1) 6% Gapapentin in Lipoderm is helpful in vulvodynia. Interesting how they made it up.
Obstet Gynecol. 2008 Sep;112(3):579-85.
Topical gabapentin in the treatment of localized and generalized vulvodynia.
Boardman LA, Cooper AS, Blais LR, Raker CA.
https://journals.lww.com/greenjournal/Fulltext/2008/09000/Topical_Gabapentin_in_the_Treatment_of_Localized.12.aspx
abstract
- Lifelong accumulative incidence 15% of vulvodynia
- Interesting formulation: – “gabapentin cream by dissolving gabapentin powder in ethoxy diglycol, then levigating the mixture into PCCA Lipoderm base (PCCA, Houston, TX), an enhanced base which facilitates tissue penetration, and placing the final product in plastic tubes for dispensation.”
- They tried varying strengths 2% to start to check for irritation and work up to 6% apply the size of a pea TID (3X/day)- after 90 days still 93% bioavailablity.
- Older, previous children and hysterectomy history are risk factors for generalized form
- 14% discontinued because of irritation or urinary symptoms 80% at least 50% improvement and 29% complete relief after 8 weeks
- reduced touch test results to 1/3rd
2) Lidocaine 5%:
Zolnoun, Denniz A; Hartmann, Katherine E; Steege, John F.
Overnight 5% lidocaine ointment for treatment of vulvar vestibulitis.
Obstetrics & Gynecology. 102(1):84-7, 2003 Jul.
https://s3.amazonaws.com/academia.edu.documents/44797551/Overnight_5_lidocaine_ointment_for_treat20160416-2366-1l1ejlz.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1546724142&Signature=KvDY4buHtf4eQEXqIpiUst1HyGI%3D&response-content-disposition=inline%3B%20filename%3DOvernight_5_lidocaine_ointment_for_treat.pdf
- “Patients were instructed to apply a copious amount of 5% lidocaine ointment to the affected area at bedtime and were asked to place a cotton ball generously coated with the 5% lidocaine ointment in the vestibule to assure continuing overnight application. We instructed patients to use the treatment nightly, for 8 or more hours.”
- VAS pain fell from 2.7/10 to 1.7 and pain with intercourse fell from 7.6/10 to 3.7
- Decline in VAS was not great but neither was pain to start with – so hard to compare both trials.
3) Nitroglycerin
J Gend Specif Med. 2002 Jul-Aug;5(4):21-7.
Safety and efficacy of topical nitroglycerin for treatment of vulvar pain in
women with vulvodynia: a pilot study.
Walsh KE, Berman JR, Berman LA, Vierregger K.
Walsh, Kathleen E., et al.
Safety and efficacy of topical nitroglycerin for treatment of vulvar pain in women with vulvodynia: a pilot study.
The journal of gender-specific medicine: JGSM: the official journal of the Partnership for Women’s Health at Columbia 5.4 (2002): 21-27.
https://europepmc.org/abstract/med/12192883
- 0.2% cream at least 3 times week 5-10 minutes prior to intercourse
- 0.2% cream at least 3 times week 5-10 minutes prior to intercourse pain improved from 7.9/10 to 5.1; with sex 7.3/10 to 4.3
- one would have thought more regular use more beneficial… Headaches has got to be an issue though regular use could relieve that.
4) Capsaicin 0.025% in acid mantle cream (chosen because it is alcohol free). 2% lidocaine gel was put one for 10 minutes prior to capsaicin. done once daily for 20 minutes for 12 weeks
Steinberg, Adam C., et al.
Capsaicin for the treatment of vulvar vestibulitis.
American journal of obstetrics and gynecology 192.5 (2005): 1549-1553
https://www.sciencedirect.com/science/article/pii/S0002937804018599
- Interested in any experience with that…
- localized forms dropped from average 7.9/10 to 2.7; generalized from 5.8 to 2.0
5) amitriptyline 2%/baclofen 2% cream (ABC)
Nyirjesy, Paul, et al.
Topical amitriptyline-baclofen cream for the treatment of provoked vestibulodynia. Journal of Lower Genital Tract Disease 13.4 (2009): 230-236.
https://journals.lww.com/jlgtd/Abstract/2009/10000/Topical_Amitriptyline_Baclofen_Cream_for_the.8.aspx
- 38 patients, with a median follow-up of 33 weeks
- 29% patients reported no or little (<30%) improvement, 18% reported moderate (30-60%) improvement, and 53% reported much (>60%) improvement
total of 71% response rate
6) meloxicam 0.3% and lidocaine 5%
Early experience with topical meloxicam and lidocaine combination for the treatment of vulvodynia.
Canadian Urological Association Journal 12.8 (2018).
http://www.cuaj.ca/index.php/journal/article/viewFile/4976/3581
- Meloxicam – selective COX-2 inhibitor with low molecular mass and high tissue tolerability
- use 5 cc applied to vulvar area BID.
- burning and stinging were side effects which made me think they used lidocaine HCL
- make the point that “because of a lack of high power studies for the efficacy of topical steroids and a significant side effect profile, the use of steroids is currently not recommended to treat vulvodynia”
- six had a subjective improvement though I suspect it could of been better if lidocaine had been ph balanced better
7) Topical estrogens and testosterone:
Sex Med. 2013 Aug;1(1):30-3. doi: 10.1002/sm2.4.
The treatment of vestibulodynia with topical estradiol and testosterone.
Burrows LJ et al.
https://onlinelibrary.wiley.com/doi/pdf/10.1002/sm2.4
- topical estradiol 0.03% and testosterone 0.01% to the vestibule twice daily
- (our compounding pharmacy makes it up in cosmetic HRT)
Surprising benefits:
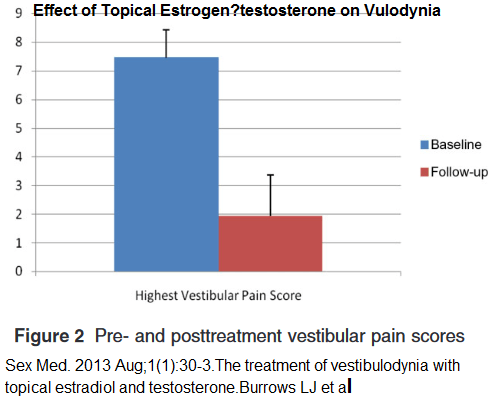
They present a before and after pic that really makes a hard sell:

A recent review of treatments did not end up recommending anything:
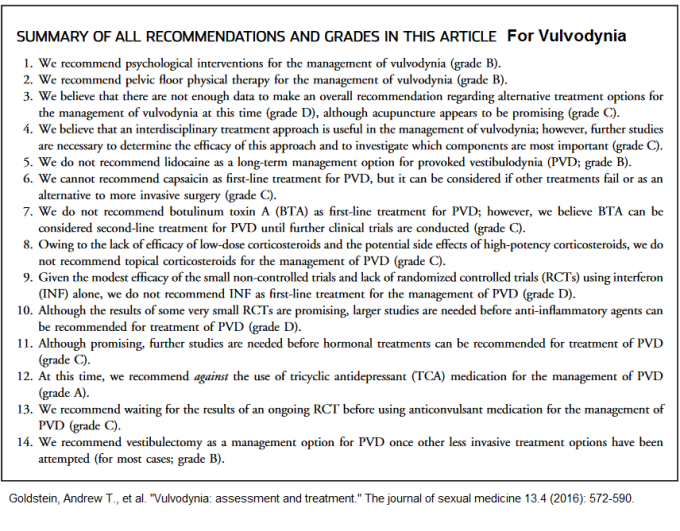
It slays me that they talk of only using “magic” for treatment – they will recommend physiotherapy and multidisciplinary without explaining what specifically why – besides the fact they are “magic”. News to you – they are not magic and unless they specify specific physio modalities their recommendations are useless… So called multidisciplinary treatment programs often work in isolation of each other and do not get any magical results. I can see lidocaine being too acidic and burning to use but would not discount gabapentin nor the hormones.
One article:
Kennedy, Colleen M., Catherine M. Leclair, and Lori A. Boardman.
Topical and injectable therapies for vulvar pain.
Female Sexual Pain Disorders (2009): 156.
http://tuleoffice.com/images/editor/File/pdf/book/IMPOTENCY/5%20(2).pdf#page=172
states:
“Some vulvodynia experts believe that compounding amitriptyline and gabapentin into topical formulations has significant potential in the treatment of vulvar pain syndromes”
Comment – so perhaps try
estradiol 0.03% and testosterone 0.01% to the vestibule twice daily
amitriptyline 2% and gabapentin 2-6% three times daily
– having to first dissolve the gabapentin in ethoxy diglycol, then levigating the mixture into PCCA Lipoderm base (PCCA, Houston, TX) makes it a bother though…
If the vulvodynia is quite localized, capsaician might be useful as well
addendum: Oral gabapentin – not really much
Effect of gabapentin on sexual function in vulvodynia: a randomized, placebo-controlled trial
Bachmann, Gloria A.Dawicki, Diane et al.
American Journal of Obstetrics & Gynecology , Volume 220 , Issue 1 , 89.e1 – 89.e8, Jan 2019
https://www.ajog.org/article/S0002-9378(18)30905-0/pdf
33 cases in gabapenin and 33 placebo cases
tenderness of vulvar vestibule with sex or touch, (ie. tampon insertion),
mean score 4/10 on VAS severity
they worked up to mean daily dose of 2476 +/- 866 mg
It was totted as successful though pain rating differences were:
Pain <4 prior: after: control – 2.7 ; gabapentin 2.6 pain >5 prior
Control 2.2 after; gabapentin 2.7 !!!
Comment – had scales which add factors repeatedly to maximize subtle changes and claimed to get benefit but pain-wise I’m not seeing it at all – if anything, the more severe subjects were worse off in the end. So basically skip oral gabapentin.
